
GP Referral Guide
Ultrasound Ireland provides comprehensive diagnostic imaging to support your clinical management plans. We are an ultrasound-focused private provider offering a full spectrum of general, obstetric, and medical diagnostic ultrasound services.
HealthLink
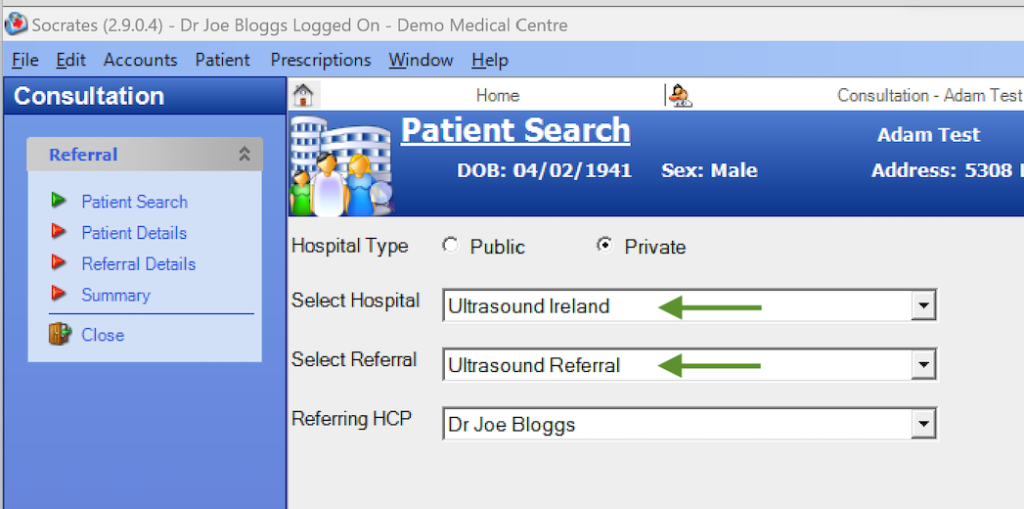
We are listed on HealthLink as Ultrasound Ireland. This is the most efficient method for secure transfer.
Secure Email
You may email referrals via HealthMail to: hello@ultrasound.ie
Paper / Patient Hand-Over
You may provide the referral letter directly to the patient, who can then contact us to schedule their appointment.
Urgent Referrals
We reserve slots for acute presentations. For immediate appointments, please call our clinical desk directly:
01 210 0232Reporting & Results
We understand that timely reporting is essential for patient management.
Urgent Findings
In the event of acute or urgent pathology, we will contact your practice immediately by telephone to convey findings, ensuring no delay in patient care.
Routine Reports
Reports with no urgent findings are issued promptly via HealthMail email or post to your practice.
Patient Preparation Guide
To ensure the highest quality images, please advise your patients of the following preparation protocols.
| Examination Type | Patient Preparation Required |
|---|---|
| Abdominal & Renal | Fasting RequiredFasting is required. Patients must fast for at least 6 hours prior to the appointment. |
| Pelvic (Male & Female) | Full BladderFull bladder required. Patients should drink 500ml of water one hour prior to the scan and hold their bladder. |
| Female Pelvic (Timing) | Day 3-5Ideally, refer for scanning between Day 3 – 5 of the menstrual cycle for optimal endometrial assessment. |
| Vascular, MSK, Thyroid, Soft Tissue | No PrepNo specific preparation is required. |
Abdominal & Renal
Fasting RequiredFasting is required. Patients must fast for at least 6 hours prior to the appointment.
Pelvic (Male & Female)
Full BladderFull bladder required. Patients should drink 500ml of water one hour prior to the scan and hold their bladder.
Female Pelvic (Timing)
Day 3-5Ideally, refer for scanning between Day 3 – 5 of the menstrual cycle for optimal endometrial assessment.
Vascular, MSK, Thyroid, Soft Tissue
No PrepNo specific preparation is required.
Questions or Need Assistance?
Our clinical team is here to support you. Contact us for any queries about referrals or patient appointments.